
MS--The Infection Connection--Part 2
Answers hidden in plain hindsight.

This is the 2nd half of a two-part post about MS. In this part, I explore infections likely to cause MS. It took me 3 weeks of research—I hope it helps someone you love. Refer to Part 1 for the basics of MS, its epidemiology suggesting infection, and the lackluster outcomes from current MS treatments.
Recap of the End of Part 1
Over the four decades since 1913, when researchers first documented transmission of neurologic disease from MS patients to animals via inoculation, interest in potential infectious causes of MS exploded. Spirochetes, a type of bacteria, were repeatedly found by microscopic examination of both MS patients’ brains and animals into which MS tissue was injected. Although many replicated these findings, often only some animals got sick, whereas some researchers failed to reproduce transmission.
Spirochetes couldn’t be grown alive from MS patients or infected animals for over 40 years. That changed in 1957 when Ichelson grew live spirochetes from MS patients’ spinal fluid. This was reproduced by several researchers, and ultimately validated by Stanford University microbiologists. But as in the animal transmission studies, some failed to replicate findings to varying degrees.
Why did some researchers succeed and others fail? As with many riddles, the answers are frequently hiding in plain sight, or in this case, plain hindsight.
Animal Transmission—Hit-or-Miss #1
Injected animals only got sick sometimes—Why? Was it because infectious organisms were only sometimes present in the injection? And when they did get sick, it ranged from mild illness to paralysis and death within days—Again, why? Did some animals develop asymptomatic or minimally symptomatic infection?
Spirochetes were found in animals inoculated from MS patients with early but not late disease. This is reminiscent of syphilis, where later disease is characterized by decreased numbers of spiral forms of spirochetes, but an increase in granular forms (spirochetes have a complex life cycle), which may no longer be infectious:
“…granules from syphilomata have never caused a successful inoculation into rabbits.”
In other spirochetal infections, spiral forms can also decrease in later disease, replaced by pleomorphic or atypical forms, including granular forms. Are these less infectious similarly to syphilis granular forms? Is this why there wasn’t animal infection after inoculation from patients with late MS?
What about the spectrum of illness when animals did get sick? Could some animals develop asymptomatic or minimally symptomatic infection? My answer—Yes. There are several large families of spirochetes. Spirochaeta myelophthora was thought to be a borrelia, of the family that includes the Lyme disease bacteria. The family of treponeme spirochetes includes the syphilis bacteria—And there are countless members of both borreliae and treponemes that cause asymptomatic or minimally symptomatic infections. Differences in virulence factors between similar-appearing microbes, along with genetic differences in how our immune systems respond to them, combine to result in a bewildering span of infection: From no symptoms to serious illness.
Culturing Live Spirochetes—Hit-or-Miss #2
A study by Kurtzke et al dimmed interest in a possible spirochetal etiology for MS. They cultured spinal fluid from MS patients and compared results to controls in two labs, one in Pittsburgh, PA and one in Philadelphia, PA. Results were classified as “definitely present,” “present,” “questionable/probable,” or “negative.” For simplicity, I’ll refer to the combined first three categories as “non-negative.” The Pittsburgh lab was unsuccessful in culturing spirochetes from any patient, whereas the Philadelphia lab demonstrated multiple spirochetal cultures. Should such discrepant findings have ended the study before publication? I think so, but that didn’t occur.
The Philadelphia lab found non-negative cultures from MS patients three times more frequently than from healthy controls, which the authors didn’t find compelling because similarly high rates were found from other neurologic patients who served as additional “controls.” At that point in time, it wasn’t yet known that borrelial infections caused a wide range of neurologic diseases— In retrospect, other neurologic patients were a poor choice for controls. Although I feel that a 300% increase in culture findings from MS patients vs healthy controls was meaningful, it wasn’t as impressive as Ichelson’s results—Why?
Kurtzke et al used pooled human serum in their culture. Sterilized serum is a blood component used to provide nutrients for hard-to-culture bacteria, like many spirochetes. But serum contains antibodies against infections we’ve encountered in our lives, more so in pooled serum from multiple donors—Could this be a problem? When using serum to enhance growth of the syphilis spirochete, only serum from patients testing negative for syphilis should be used, as antibodies impair its growth.
The same holds true for Spirochaeta Myelophthora—Only serum from uninfected people should be used. But there was no antibody test to screen blood donors for this infection until 1959—And it showed that 26% of healthy people possibly harbored asymptomatic infection. So pooled human serum would likely contain antibodies against it—Attacking the bacteria rather than helping it grow. And although single donor serum would be less likely to have antibodies than pooled serum, a 26% chance would still be high enough to produce some failed cultures.
Ironically, this is the very same Kurtzke I referenced in Part 1 for his epidemiologic insights into the Faroe Islands MS epidemic. He wrote:
“We conclude that "MS" is a widespread, systemic, specific infectious disease only rarely causing neurologic symptoms...” —John F. Kurtzke
If he had believed this in 1962, would he have redesigned his culture study to exclude pooled human serum? Maybe, but it probably wouldn’t have been enough—A paradigm shift was occurring.
The End of the Golden Age of Medicine
Steroids were first used for rheumatoid arthritis (RA) in 1949. Their quick suppression of symptoms was seductive—Despite providing no cure, their use heralded the thinking of autoimmune conditions as distinct medical entities, which spilled over into how scientists viewed MS. But is it logical to believe that our immune systems, of their own accord, would start attacking us? My answer—No.
Before the dawn of the autoimmune era, it was already well-accepted that many chronic infections caused chronic inflammation. There are only so many inflammatory pathways our immune systems can take when fighting infections—So the same inflammatory disease can result in response to different microbes. For example, it’s known that syphilis can cause a clinical presentation compatible with MS. So would it be such a stretch for other spirochetes to do this as well?
A quick detour away from MS to explore RA highlights the pitfalls of the autoimmune dogma. Treatable infections have been linked to what are now typically defined as autoimmune conditions, such as RA—Tuberculosis (TB) is just one example. Even in 1958, scientists described TB arthritis as:
“…clinically and radiologically, were indistinguishable from rheumatoid arthritis.”
Many infections may contribute to, or directly cause RA, including hepatitis C, toxoplasmosis, brucellosis, bartonellosis, mycoplasmosis, and others. In my professional experience of treating many thousands of patients diagnosed with autoimmune conditions, and in my personal experience of having been one such patient, I’ve never seen a single rheumatologist check an exhaustive infectious disease panel for infections that can cause RA. I have seen them check a couple here and there, but I don’t think that’s good enough. It reminds of my ex-landscaper. I complained to him once that there were weeds growing among the rhododendrons. He said, “Sometimes I pick a weed.”
So if rheumatologists did all check a jumbo list of infections before making a diagnosis of RA, we’d be able to accurately tell who has which infection, right? It varies. For some infections it is that simple—Hepatitis C is easy to diagnose with highly sensitive tests to show both prior exposure and viral persistence. Toxoplasmosis has a decent antibody test, but it’s quite difficult to prove its persistence. Many of the other infections are caused by even more stealthy microbes, incredibly difficult to find in the body—So we rely on often unreliable antibody tests.
When the Golden Age of Medicine ended, the furious search to unlock the myriad causes of chronic illnesses changed to focus on symptom suppression, a far more profitable endeavor for pharma as patients never get cured. Over time, this has snowballed, leading to the currently orchestrated autoimmune gold rush.
Epstein-Barr Virus’ Role in MS
Epstein-Barr virus (EBV) is a pervasive herpes virus chronically infecting about 95% of US adults. Yet the rate is even higher in MS patients vs healthy controls. It’s been difficult to prove causality due to EBV’s massive prevalence in healthy people, but a study of military personnel, mostly teenagers and some young adults, showed an increased risk of MS after initial EBV infection:
“…the risk of MS increased 32-fold after infection with EBV…”
Could EBV, an ancient virus universal in all human populations, explain the Faroe Islands MS epidemics?
“the MS epidemics in the Faroe Islands cannot be explained by EBV, because almost certainly EBV was ubiquitous in the Faroe Islands, as it is in all other human populations investigated.”
EBV infection in young childhood is usually a mild illness, whereas in adolescence it often causes infectious mononucleosis. Developed areas of the world—in which EBV infection is delayed to adolescence due to better hygiene—have rates of MS 20-40 times higher than areas were EBV infection occurs in early childhood.
“…infection alone is clearly insufficient to cause MS. Age at primary infection and the host's immunological response may be modifiers of the EBV-associated risk of MS. Accordingly, infectious mononucleosis, usually caused by EBV infection in adolescence, has been associated with an increased risk of MS…”
Biologic systems are networked tangles, so studying a single variable often falls flat. For example, Lyme borrelia reactivates latent EBV—Is there a combined effect?
“…may prove a mixed borrelial and viral cause of severe neurological disease.”
There are also immune system changes that occur due to mononucleosis and remain lasting after it’s resolved. Are these changes enough to cause MS? Or do they have to work in concert with another agent? Perhaps another ubiquitous infection?
The Case For Chlamydia
Chlamydia pneumoniae is an airborne bacteria, not the sexually transmitted type. It’s a highly prevalent microbe that sets up low grade chronic infection—Implicated in a range of chronic illness, from heart disease to asthma to MS. Although chlamydial DNA and antibodies are found in spinal fluid of MS patients more often, the relationship of chlamydia to MS has been contested by some, and considered as a possible co-factor by others, particularly in progressive forms of MS.
Many years ago, I called a researcher studying chlamydia in MS patients. I asked if he treated his MS patients with antibiotics. He did. I asked if they were getting Herxheimer reactions. He said that they were—Upon starting antibiotics, their MS would get a lot worse before getting better, that it was really scary, and that antibiotics could only be used very gradually.
So I said, “But chlamydiae don’t cause Herxheimers. Have you ever tested your patients for Lyme?” After a few seconds of silence he said, “I won’t touch Lyme with a 10-foot pole.”
Spirochetes—Why is There Never a 10-Foot Pole Around When You Need One?
Spirochetes are a mysterious bunch, and the borreliae that cause Lyme are just about the most baffling. Lyme has been controversial from early on. Why? It’s difficult to cure—A Johns Hopkins study showed that 39% of Lyme patients diagnosed and treated early, when it’s easiest to cure, had persistent symptoms or functional impacts six months later. Another study found that 61% of patients stayed sick long term, again despite early treatment.
Any many don’t get diagnosed early because Lyme antibody tests are inaccurate—A review of 8 studies found that they miss more cases than they diagnose. Plus, there are new species of borreliae discovered all the time. Some fall within the wide umbrella of Lyme, but many others are far enough out on the family tree to only be cousins—testing negative by Lyme tests, but causing similar illness.
And despite being incredibly challenging to culture in the test tube, Lyme bacteria have been grown alive from patients who’ve not been cured despite months to years of antibiotics—Including from a patient who died from chronic Lyme when her medical insurance refused to cover treatment, despite CDC growing live Lyme bacteria from her spinal fluid after antibiotics failed. And to top it off, the same antibiotics which are claimed by some to easily cure Lyme, don’t kill it in the test tube.
What does this have to do with MS? A protein in borrelia spirochetes looks, to our immune systems, very similar to the insulation around nerves, called myelin. During the immune response against spirochetes, there can be antibodies formed against myelin, causing its breakdown, known as demyelination—The hallmark of MS.
Lyme can be clinically indistinguishable from MS, leading some researchers to postulate that Lyme may be a cause of MS. Some prefer to use the term “mimic” when referring to Lyme causing an illness compatible with MS—But if it’s mimicking MS, then isn’t it causing MS in that patient? The question is, how often does this occur?
Who can say?—But spirochetal round bodies, formerly known as cystic forms, were found in the spinal fluids of 10 MS patients, but not in 5 healthy controls, with the exception of one patient without symptoms but who had a history of Lyme.
Deaths from Lyme* vs deaths from MS were compiled from US Census data and plotted on these maps, county by county, across the US. This picture speaks to me.
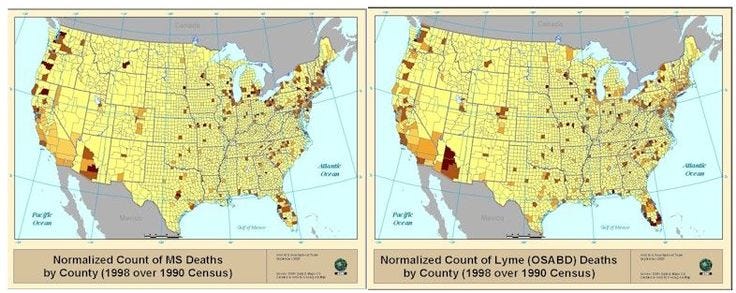
*Includes Lyme, babesiosis, and other arthropod-borne infections as they couldn’t be separated out in the data search. Since Lyme is the most common arthropod-borne infection in the US by far, this is reasonably representative of just Lyme.
Multiple open label trials with the antibiotics minocycline and doxycycline have found benefits across several metrics in MS, including improvements when standard MS treatment had failed. A randomized placebo-controlled trial evaluating the use of minocycline in patients soon after their first demyelinating episode was published in the New England Journal of Medicine. Patients were treated with minocycline vs placebo and followed over time. They found an almost 50% reduction in the risk of conversion to full MS at 6 months in the minocycline-treated group vs placebo. And in my experience, there are far more effective and safer regimens than single agent minocycline.
My two cents: I’ve treated thousands of MS patients over the years, and the large majority have responded to oral antibiotics, as well as certain non-antibiotic antimicrobials, with Herxheimer reactions followed by very material improvements. But this is a complex task with the potential for worsened MS outcomes, most especially in progressive forms. I don’t want to make it sound simpler or easier than it is—The only reason I’ve been successful is the many years of experience and lessons I’ve learned along the way. But I’m thoroughly convinced of a spirochetal etiology for most relapsing-remitting MS patients.
And I’m equally convinced of a more hopeful future for MS patients by finding and treating its cause rather than just suppressing its symptoms.
Thank you for taking the time to consider my thoughts on MS, a condition which is very personal to me. I’m extra-appreciative to those who’ve opted for the paid subscriptions. For those who are new here, please don’t forget to like and subscribe. If you think what you’ve read here today can help someone in need, please share it widely.
Disclaimer: None of my posts contain medical advice. These posts are intended for purely informational purposes only. Please check with your doctor before undertaking any course of treatment.
I will be forever grateful to my friend, who in their personal blog, wrote: “Multiple Sclerosis is Lyme Disease: Anatomy of a cover up”. https://owndoc.com/lyme/multiple-sclerosis-is-lyme-disease-anatomy-of-a-cover-up/
Having been diagnosed as Multiple Sclerosis, 10 years ago, reading about what’s known about the condition, lots of things didn’t quite make sense to me. I had however started feeling sick with that felt like an infection a year ago, so upon looking into what kind of infections could cause similar findings as the MS “syndrome”, bam, there it was, lots of controversy. It then introduced me to Thomas Grier, the Brorson brothers, Alan Macdonald. most of it started to make sense.
Taking my own decision and risk, I went late to a pharmacy, and asked for Doxycicline. I said that I had forgotten my prescription. Thankfully, by not living in US at the time, that worked. And swallowed straight 500mg of generic Doxy.
What ensued was a nightmare, High fever, shaking, full on hives, tachycardia, green stuff coming out of my mouth, and a long list of other symptoms. That was the beginning of a long journey of discovery, with many wins, but many failures. 10 years later, I am reading this and thinking how blessed I was that afternoon, 10 years ago, that someone had decided to synthesize this info for the public to ingest. Thank you Dr. Philips, this kind of thing helps more than you could know.
Fascinating, thanks!
I suspect a connection between high levels of senescent cells and MS. Senescent cells consume high levels of NAD+, dramatically reducing what's available for other needs. The primary issue is high levels of CD38 in senescent cells. https://pubmed.ncbi.nlm.nih.gov/27304511/
Minocycline is interesting because it has senolytic effects, and is also anti-inflammatory. https://www.frontiersin.org/articles/10.3389/fnagi.2019.00143/full
Terri Wahls treats MS with diet, prescribing large amounts of veggies. These are good sources of apigenin, which blocks CD38 and allows normal NAD+ levels. I've been wondering if this is a major part of her success (plus dramatically lower inflammation in the short/medium-term).
I'd be curious if your MS patients improve with apigenin, especially with liposomal forms. Fisetin is an excellent/safe senolytic, for patients under 65 or so, can be used in high doses for 2-4 days per month... Glycine is depleted by chronic inflammation, so supplementation helps improve glutathione levels and reduce inflammation. High lysine to arginine also suppresses viral growth, so if EBV or other chronic viral infections are a problem this would help.
Stephen Buhner is a rare combination of medical scientist and herbalist; he has a lyme protocol that is quite effective: https://www.amazon.com/Healing-Lyme-Borreliosis-Coinfections-Rickettsiosis/dp/0970869649